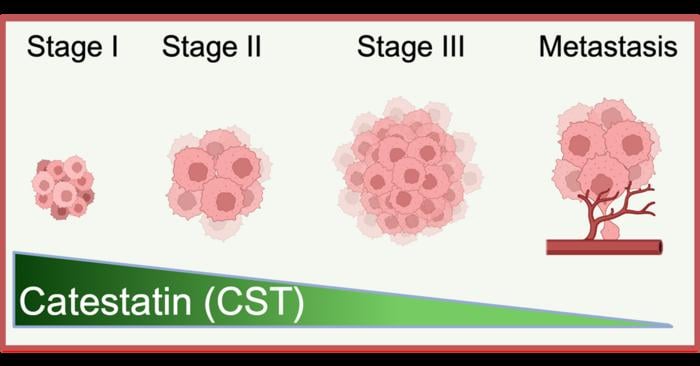
Somewhere within your skin at this moment, a tiny protein fragment is performing its functions. It aids in managing inflammation. It contributes to wound healing. Moreover, it appears to be subtly curtailing the kind of cellular disorder that can lead to melanoma. This molecule is known as catestatin, and until very recently, no one considered examining its behavior in skin cancer. When researchers at UC San Diego finally took a closer look, they discovered what seemed like a hint: as melanoma evolves into more aggressive phases, levels of catestatin decrease. This pattern was consistent among patient after patient.
The implication, if substantiated, is unsettling in a particular manner. The body, it appears, may already possess the means to combat this cancer. The tumor learns to mute the defense.
Catestatin originates from a larger protein known as Chromogranin A, or CgA, which you might not be familiar with but actually has numerous functions. CgA is implicated in cardiovascular regulation, immune signaling, metabolic control, and neuroendocrine communication; it’s one of those proteins that seems omnipresent once you start paying attention, which perhaps explains why the peptide fragment it generates has been overlooked in oncological research for so long. Researchers have investigated catestatin’s involvement in blood pressure, in inflammation, in the peculiar physiology of stress response. Cancer? Not as much.
Sushil K. Mahata, a professor of medicine at UC San Diego and a research physiologist at the VA San Diego Healthcare System, changed this narrative. His team observed that catestatin showed up in skin tissue and began questioning its potential roles there, particularly regarding melanoma. What ensued was an experimental momentum where each discovered answer spawned three additional inquiries.
Upon restoring catestatin to melanoma cells derived from patients in laboratory settings, the cells exhibited responses that were, frankly, remarkable. They began undergoing programmed cell death, known as apoptosis. They ceased proliferating at their regular pace. They became less invasive and less likely to migrate like metastatic cancer cells do. Simultaneously, normal skin fibroblasts present in the same experimental setting remained largely unaffected. In other words, the peptide seemed to selectively target tumor cells without harming the surrounding healthy tissue.
“Melanoma is particularly perilous because tumor cells can adapt and develop resistance to treatments. Our research indicates that CST can disrupt those pathways of resistance and redirect melanoma cells toward a more manageable state,” stated Mahata.
That latter point regarding resistance might be where the findings become genuinely intriguing from a clinical perspective. Drug resistance is what ultimately allows melanoma to be fatal. Vemurafenib, a targeted treatment that operates by inhibiting a mutated variant of a protein called BRAF, can initially yield remarkable results. Then, frequently within months, the cancer finds ways to bypass it; the cells activate alternative survival mechanisms, upregulate stress-response genes, and remodel the extracellular matrix to create a more favorable microenvironment. What catestatin seems to accomplish, at least in lab settings with Vemurafenib-resistant cell lines, is shutting off some of those pathways. Transcriptomic profiling indicated downregulation of genes associated with hypoxia signaling, in the epithelial-to-mesenchymal transition that facilitates cancer spread, and in the molecular machinery responsible for stress adaptation. Several specific mediators, including proteins related to extracellular-matrix remodeling and growth factor signaling, were also suppressed. It’s a comprehensive sweep, which could be viewed as optimistic or complex based on perspective.
In mouse models, the outcomes were reasonably promising. Animals treated with catestatin exhibited significantly reduced tumor growth and overall tumor load, with no observable systemic toxicity. Yes, these are rough figures, and mouse models are notoriously imperfect mimics for human cancer. However, the absence of toxicity is, at the very least, a solid starting point.
Satadeepa Kal, the postdoctoral researcher who led the investigation, highlighted something worth contemplating. “In an age of small-molecule inhibitors and immunotherapy, the therapeutic possibilities of peptides remain comparatively underexplored,” she remarked. “Our study illustrates that peptide-based therapies may present a potent approach not only against melanoma and drug resistance but potentially against other cancers and intricate metabolic diseases as well.” Peptides occupy a unique position in pharmacology: more specific than traditional chemotherapy (which tends to affect all rapidly dividing cells), more targetable than many small molecules, yet historically challenging to produce and administer consistently. The field has been progressing slowly over the years.
There are, of course, caveats. Numerous ones. The gap between a promising finding in cell lines and mouse models and a tangible clinical treatment is typically measured in years, sometimes even decades, and many candidates never reach that stage. Whether catestatin can be developed into a stable, deliverable medication that maintains its selectivity in the considerably messier environment of a human tumor remains an open question.